40 years old male came for ultrasound with c/o painful swelling over anterior abdominal wall since 2 days. Pt had history of severe cough. No history of trauma.
Findings and discussion:
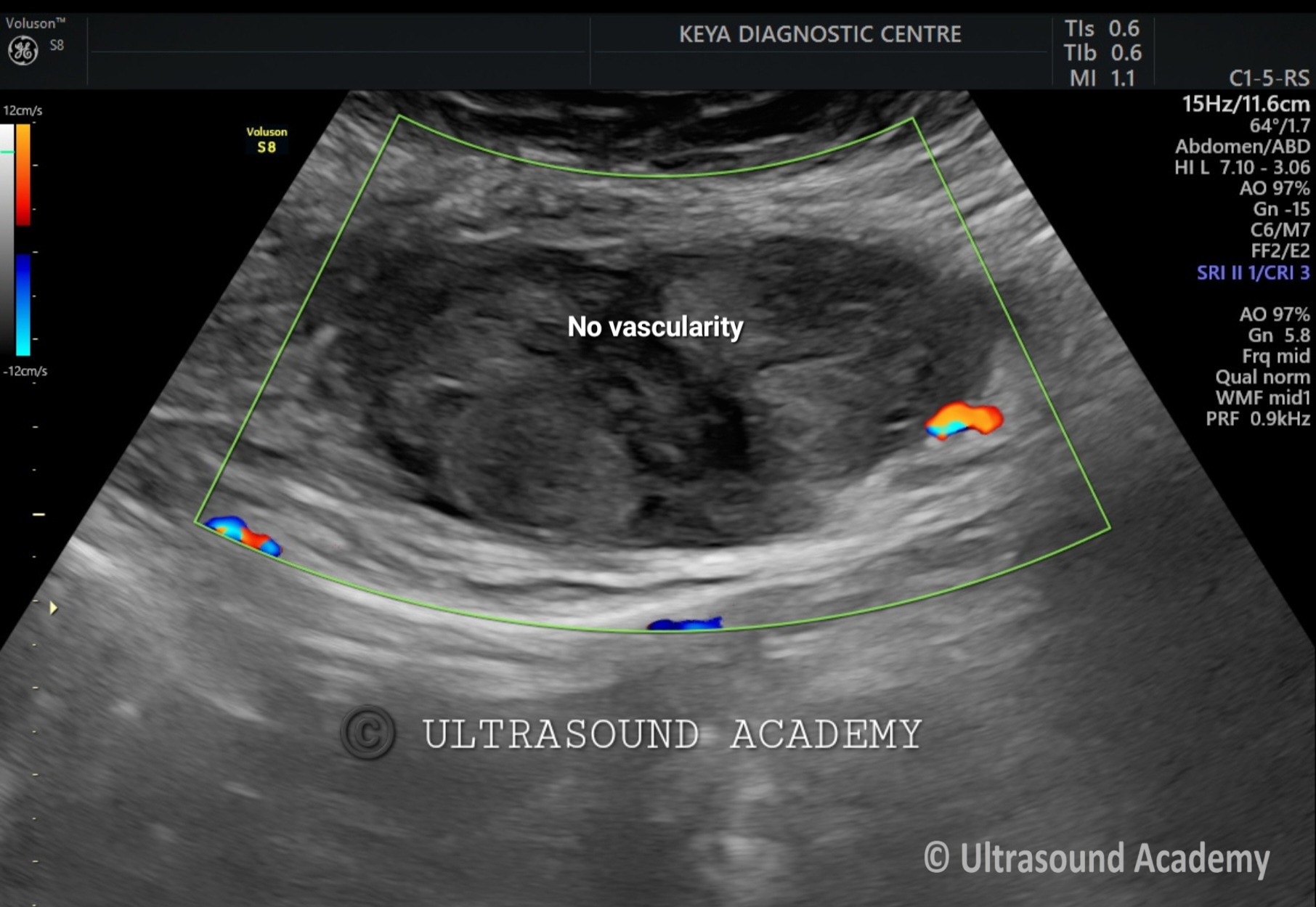
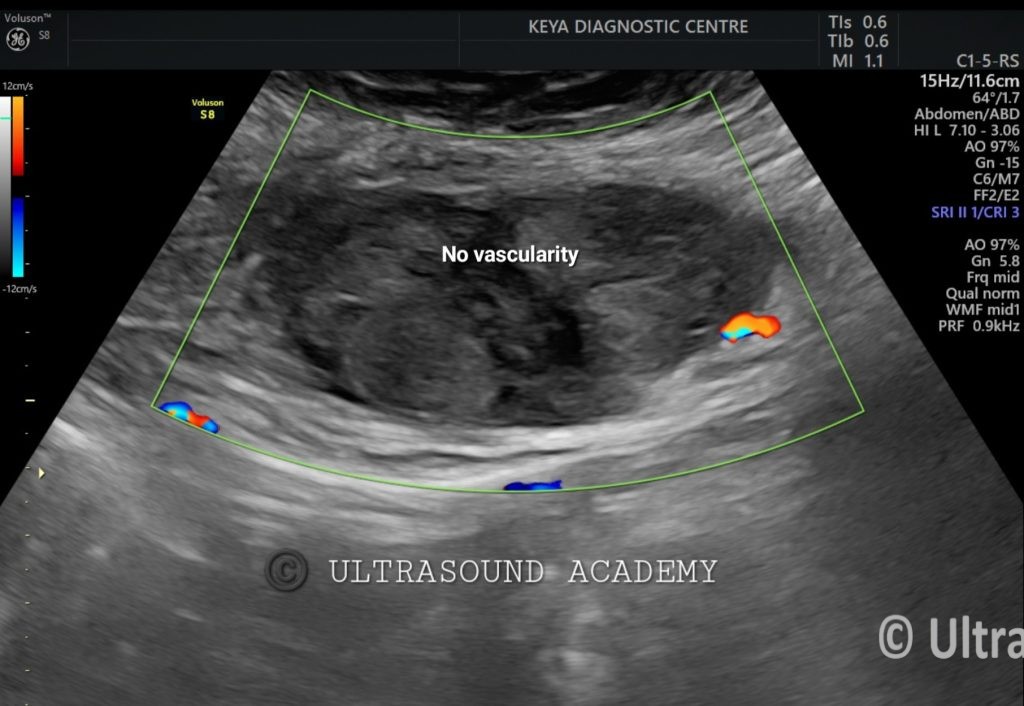
On B mode ultrasound:
There is well defined heterogenous predominantly hyperechoic lesion/ area is seen involving the left rectus abdominis muscle. No intra- abdominal extension is noted.
On Color Doppler examination: No vascularity noted.
So, the diagnosis of acute rectus abdominis muscle hematoma is given.
Rectus hematoma may occur in patients:
I) On anticoagulation medication
II) with a known coagulopathy
III) following abdominal wall trauma.
Rectus Abdominis Muscle Hematoma on Ultrasound
A rectus abdominis muscle hematoma is a collection of blood within the rectus abdominis muscle, usually due to trauma, anticoagulation therapy, excessive strain, or abdominal surgery. Ultrasound (USG) is often used as an initial imaging modality to diagnose and assess the extent of the hematoma.
Ultrasound (USG) Findings of Rectus Abdominis Muscle Hematoma:
Early Phase (Acute Hematoma – Fresh Bleed)
Hyperechoic or mixed echogenicity mass within the rectus abdominis muscle.
Poorly defined margins due to active bleeding or edema.
No significant posterior acoustic enhancement.
Intermediate Phase (Subacute Hematoma – Few Days to Weeks)
Becomes more hypoechoic due to clot breakdown.
May have internal septations or a heterogeneous appearance.
Fluid-fluid levels may be seen if re-bleeding occurs.
Late Phase (Chronic Hematoma – Weeks to Months)
Hypoechoic to anechoic well-encapsulated collection.
Possible calcifications or fibrosis.
Can mimic an abscess or cystic mass.
Doppler Ultrasound Features:
No significant internal vascularity (distinguishes hematoma from tumors).
Perilesional hyperemia if inflammation or infection is present.
Differential Diagnosis:
Abdominal wall abscess (may show internal echoes and hypervascularity on Doppler).
Hernia (shows peristalsis and movement with Valsalva maneuver).
Tumor/mass (may have internal vascularity and solid components).
Clinical Correlation & Next Steps:
History of trauma, coughing, anticoagulant use, or exercise is key.
CT or MRI may be needed for better characterization if USG findings are unclear.
Conservative management (rest, analgesia, compression) for stable hematomas.
Intervention (drainage or surgery) in cases of large, expanding, or infected hematomas.